Shropshire baby deaths: Hospitals must adopt new safety steps
- Published

Donna Ockenden, a former senior midwife, is leading the review into maternity care in Shropshire
All NHS trusts in England have been given a deadline of Monday to enact safety improvements in maternity care amid Shropshire's baby deaths scandal.
Heath chiefs have told hospitals they must have the 12 "urgent clinical priorities" in place by 17:00 GMT.
The move is to address "too much variation" in outcomes for families.
It comes during a probe into the maternity care of more than 1,800 families in Shropshire.
The inquiry, launched amid concerns of repeated failings at Shrewsbury and Telford Hospital NHS Trust (SaTH), focuses on the experience of 1,862 in total, and includes instances of infant fatality.
An interim report published last week found poor care over nearly two decades had harmed dozens of women and their babies.
The report called for seven "essential actions" to be implemented at maternity units across England.
But that has since been transformed into 12 clinical tasks, including giving women with complex pregnancies a named consultant, ensuring regular training of fetal heart rate monitoring, and developing a proper process to gather the views of families.
The directions are revealed in a letter seen by the BBC in which NHS England says there is "too much variation in experience and outcomes for women and their families".

Donna Ockenden is leading the inquiry into maternity standards at SaTH, which runs Royal Shrewsbury Hospital and Telford's Princess Royal Hospital.
On Tuesday she told MPs the trust had consistently failed to identify the main cause of maternity failings.
The Commons Health and Social Care Committee also heard another of the interim report's conclusions, that some mothers were blamed for babies' deaths.
Ms Ockenden said that amid the "culture" of blame there was parental guilt, and failure to listen to families "stood out" above all issues.
And she added there was a dual culture of focusing on natural births almost at "any cost".
The majority of incidents investigated occurred between 2000 and 2019.
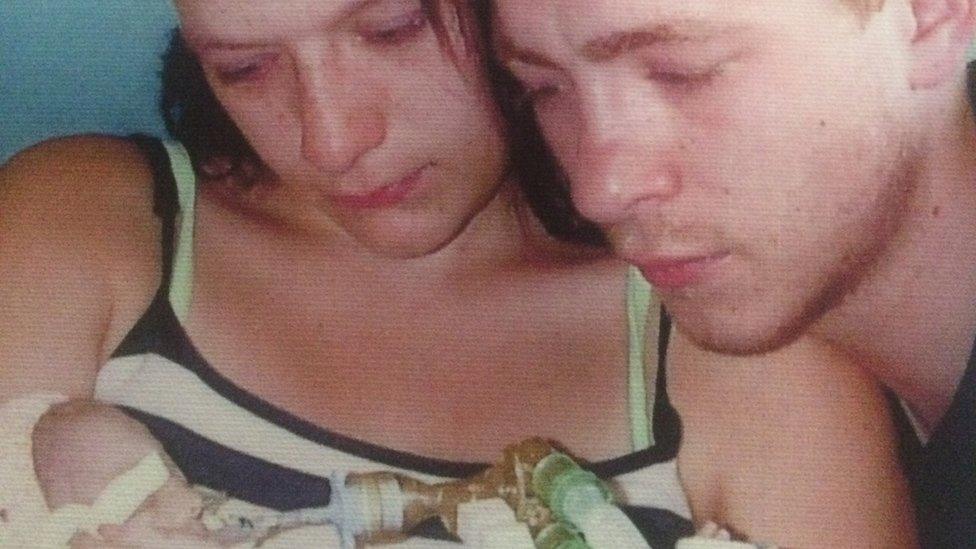
WATCH: The parents of babies Kate and Pippa talk about the pain of losing their child
Ms Ockenden told MPs that when the trust did investigate an issue "they often just hung their hat on the wrong hook".
She said: "They picked something that certainly wasn't the cause and got diverted - they failed to learn."
She also told the committee: "I think the one issue that stands out above everything else was a failure to listen to families.
"We've come across a lot of families who tried really hard to get the system - the trust - to listen to them.
"They carry on their shoulders a large amount of guilt now because they feel they failed to get the system to listen to them."
The interim report lists numerous traumatic birth experiences including the deaths of babies due to excessive force of forceps and stillbirths that it says could have been avoided.
MPs heard on Tuesday there was a focus on natural birth "at pretty much any cost".
Ms Ockenden said: "There were times, there were cases, had a baby been delivered by a Caesarian section, the outcome may well have been better and almost certainly safer."
She also told the hearing her investigation had uncovered "lots of examples of dismissive letters, very unkind letters".
She said: "There was also a culture of 'this is your fault' to the mothers - 'if you hadn't done X, your baby may have lived'."
Following its publication last week, the chief executive of SaTH said the trust was committed "to implementing all of the report's actions".

Follow BBC West Midlands on Facebook, external, Twitter, external and Instagram, external. Send your story ideas to: newsonline.westmidlands@bbc.co.uk , external
- Published10 December 2020

- Published21 July 2020

- Published1 July 2020
- Published30 June 2020

- Published30 June 2020

- Published16 January 2020

- Published29 November 2019

- Published26 November 2019
- Published19 November 2019
- Published12 April 2017








